372
CHAPTER 26
amongst workers in this field. There is, however, now the tendency to perform TUR at
an earlier date than was the rule previously, although as early as 1947 Bumpus
et al.
advocated TUR in upper motor neuron lesions 2-6 weeks after return of reflex activity
of the spinal cord had occurred. Bors & Comarr (1971) are now inclined to perform TUR
after three months—when intermittent catheterization fails to establish satisfactory
micturition in paralysed patients with lower motor neurone lesions. While I agree that
TUR should not be delayed for long, I am not in favour of any dogmatism regarding the
time for TUR performance. Having regard to the great variability of bladder dysfunction
in paraplegics and tetraplegics and the varying speed of the patient's adjustment to his
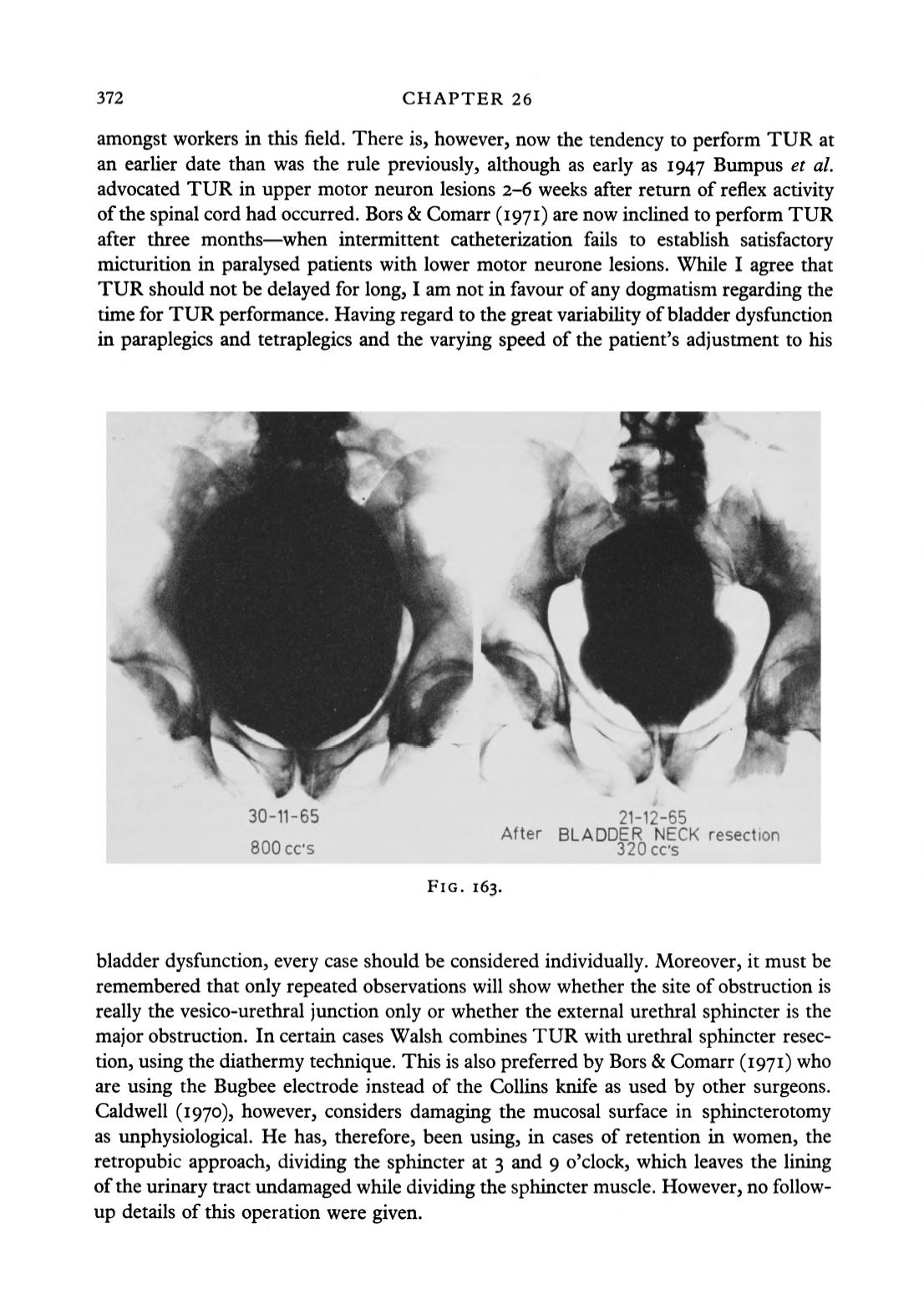
30-11-65
SOOcc's
21-12-65
After BLADDER NECK resection
320cc's
FIG. 163.
bladder dysfunction, every case should be considered individually. Moreover, it must be
remembered that only repeated observations will show whether the site of obstruction is
really the vesico-urethral junction only or whether the external urethral sphincter is the
major obstruction. In certain cases Walsh combines TUR with urethral sphincter resec
tion, using the diathermy technique. This is also preferred by Bors & Comarr (1971) who
are using the Bugbee electrode instead of the Collins knife as used by other surgeons.
Caldwell (1970), however, considers damaging the mucosal surface in sphincterotomy
as unphysiological. He has, therefore, been using, in cases of retention in women, the
retropubic approach, dividing the sphincter at 3 and 9 o'clock, which leaves the lining
of the urinary tract undamaged while dividing the sphincter muscle. However, no follow-
up details of this operation were given.


