F- CLINICAL ASPECTS OF SPINAL CORD INJURIES
467
were applied (Dr A.Moolgaoker), and a healthy premature male infant weighing 5 Ib
8 oz was delivered at 1.56 p.m. The placenta was delivered at 2 p.m. and the episiotomy
was repaired. The headache was most intense during delivery, then disappeared, returned
during delivery of the placenta, disappeared again and was replaced by a moderate pain
in the back of the neck with slight stiffness which lasted 20 min.
No drugs were given, apart from an i.m. injection of i ml of syntometrine given with
delivery of the anterior shoulder. No local anaesthetic was given for repair of the episio
tomy; the insertion of each suture produced a strong contraction of the anal sphincter
but there were no subjective sensations and no rise in BP.
Fig. 193 demonstrates the changes in blood pressure and pulse rate before, during
and after delivery.
The cardiac irregularities developing during the various stages of labour could be re
corded electrographically and were of special interest in this case. They were as follows:
At i p.m., during a uterine contraction, an irregularity of the pulse was first noted;
clinically, this seemed to be due to extra-systoles. E.C.G. recordings started at 1.25 p.m.
During the rest of the labour, a number of arhythmias were recorded, which are demon
strated in detail in Figs. I93a-g. Various arhythmias were demonstrated, starting with
prolongation of the P-R interval with regular ventricular extra-systoles (Figs. 1933, b, c)
followed by 2nd degree A-V block with A-V escape beats (Fig. 1936). On occasions,
when there was only a moderate rise of blood pressure, a bradycardia with normal sinus
rhythm was found (Fig. I93d). As the hypertension increased (1.52 p.m., Fig. I93f),
2nd degree A-V block returned and there were ventricular extra-systoles differing in
shape and direction from those previously seen (Fig. I93c). During the actual delivery,
the P waves disappeared and regular ventricular extra-systoles occurred firstly at every
third beat (Fig. I93g) and later at every alternate beat (Fig. I93h).
As soon as the baby had been delivered, the electrocardiogram became normal,
except that during the delivery of the placenta there were two more ventricular extra-
systoles (Fig. 1931). The three standard leads after delivery are shown in Fig. I93g.
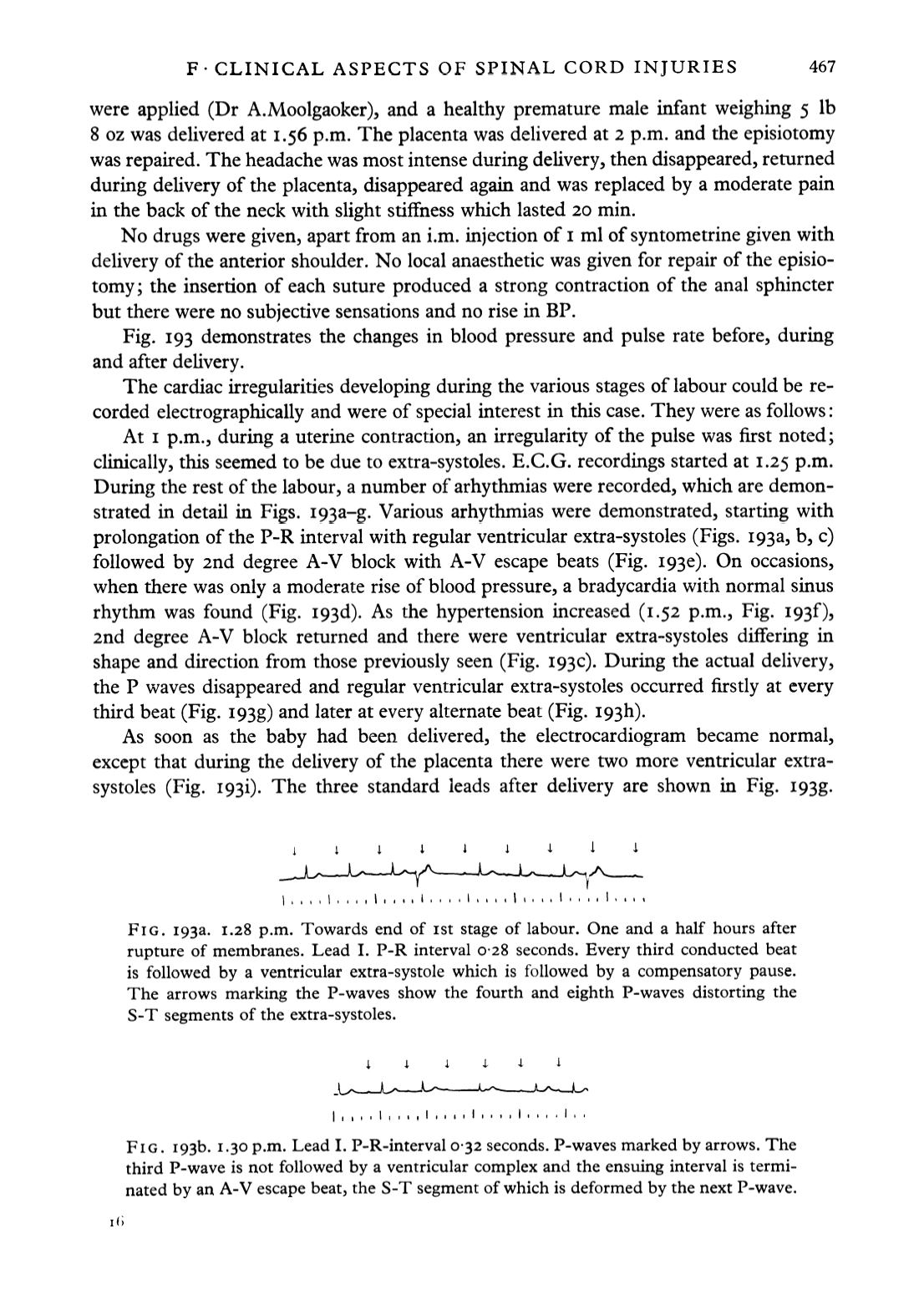
FIG. 1933. 1.28 p.m. Towards end of ist stage of labour. One and a half hours after
rupture of membranes. Lead I. P-R interval 0-28 seconds. Every third conducted beat
is followed by a ventricular extra-systole which is followed by a compensatory pause.
The arrows marking the P-waves show the fourth and eighth P-waves distorting the
S-T segments of the extra-systoles.
FIG. i93b. 1.30 p.m. Lead I. P-R-interval 0-32 seconds. P-waves marked by arrows. The
third P-wave is not followed by a ventricular complex and the ensuing interval is termi
nated by an A-V escape beat, the S-T segment of which is deformed by the next P-wave.


