512
CHAPTER 30
In tetraplegics below C5, occasionally a sore may develop over the elbow. Partial
resection of the infected olecranon process and its bursa may be necessary.
PRE-OPERATIVE MANAGEMENT
There was a time when plastic surgeons were keen to perform rotation or transposition
flaps in sores with active infection and were quite satisfied if the flap was taken by 50,
60 or 80 per cent. We always considered this as a 100 per cent failure as by such results
an open septic wound was transformed into an undermined one. However, it is now
generally agreed that surgical repair of sores in paraplegic patients should not be under
taken unless the active infection, in particular, of staphylococci and haemolytic strepto
cocci, is controlled, the sore is healing and the general condition of the patient is perfect.
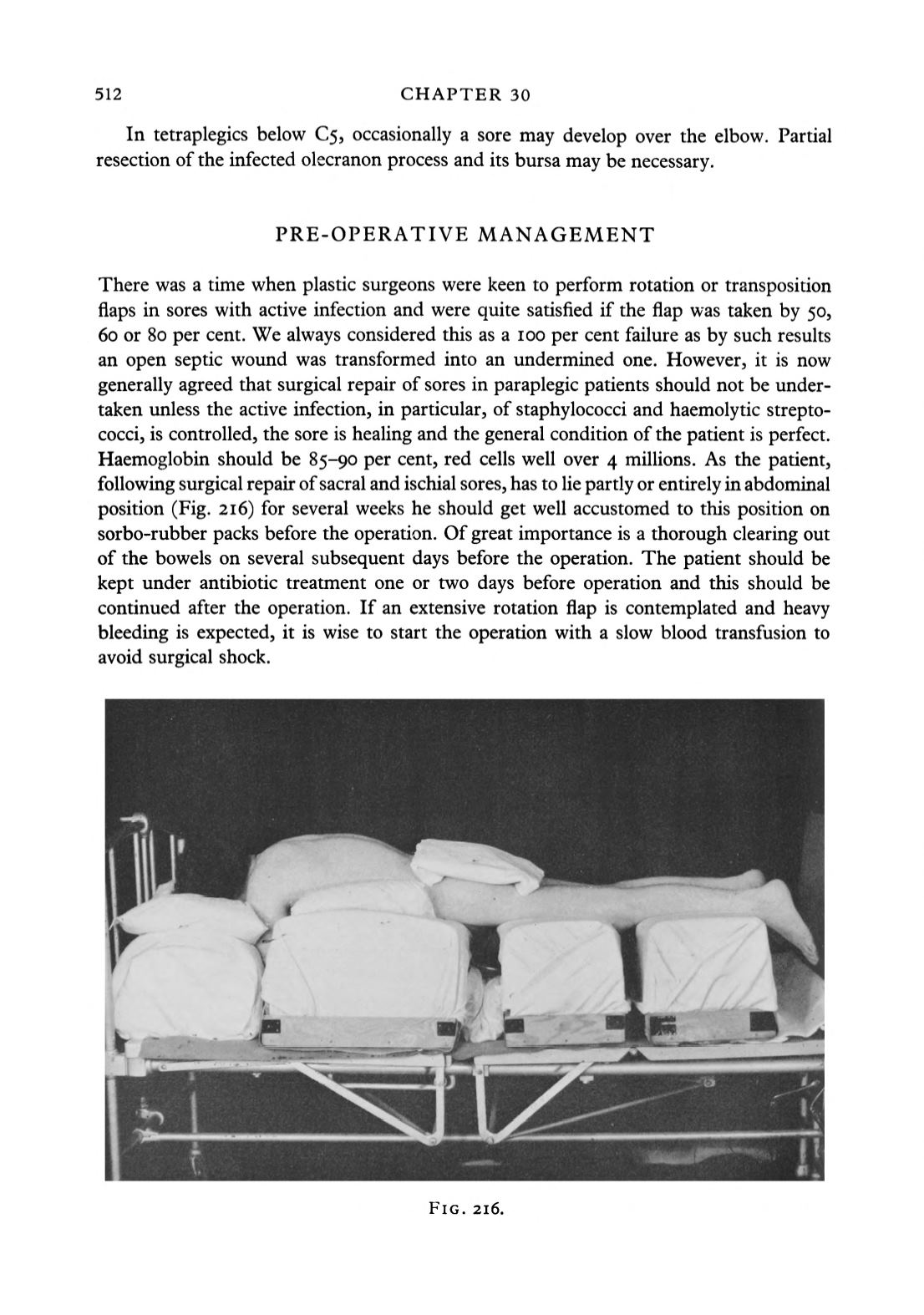
Haemoglobin should be 85-90 per cent, red cells well over 4 millions. As the patient,
following surgical repair of sacral and ischial sores, has to lie partly or entirely in abdominal
position (Fig. 216) for several weeks he should get well accustomed to this position on
sorbo-rubber packs before the operation. Of great importance is a thorough clearing out
of the bowels on several subsequent days before the operation. The patient should be
kept under antibiotic treatment one or two days before operation and this should be
continued after the operation. If an extensive rotation flap is contemplated and heavy
bleeding is expected, it is wise to start the operation with a slow blood transfusion to
avoid surgical shock.
FIG. 216.


