150
CHAPTER 12
(e) Once the patient is out of bed and mobile, it is not unusual for the plates to become
loose so that they cut out of the spinous processes, and have to be removed. This is in
accordance with Holdsworth's own experience (Holdsworth, 1963), but in our experience
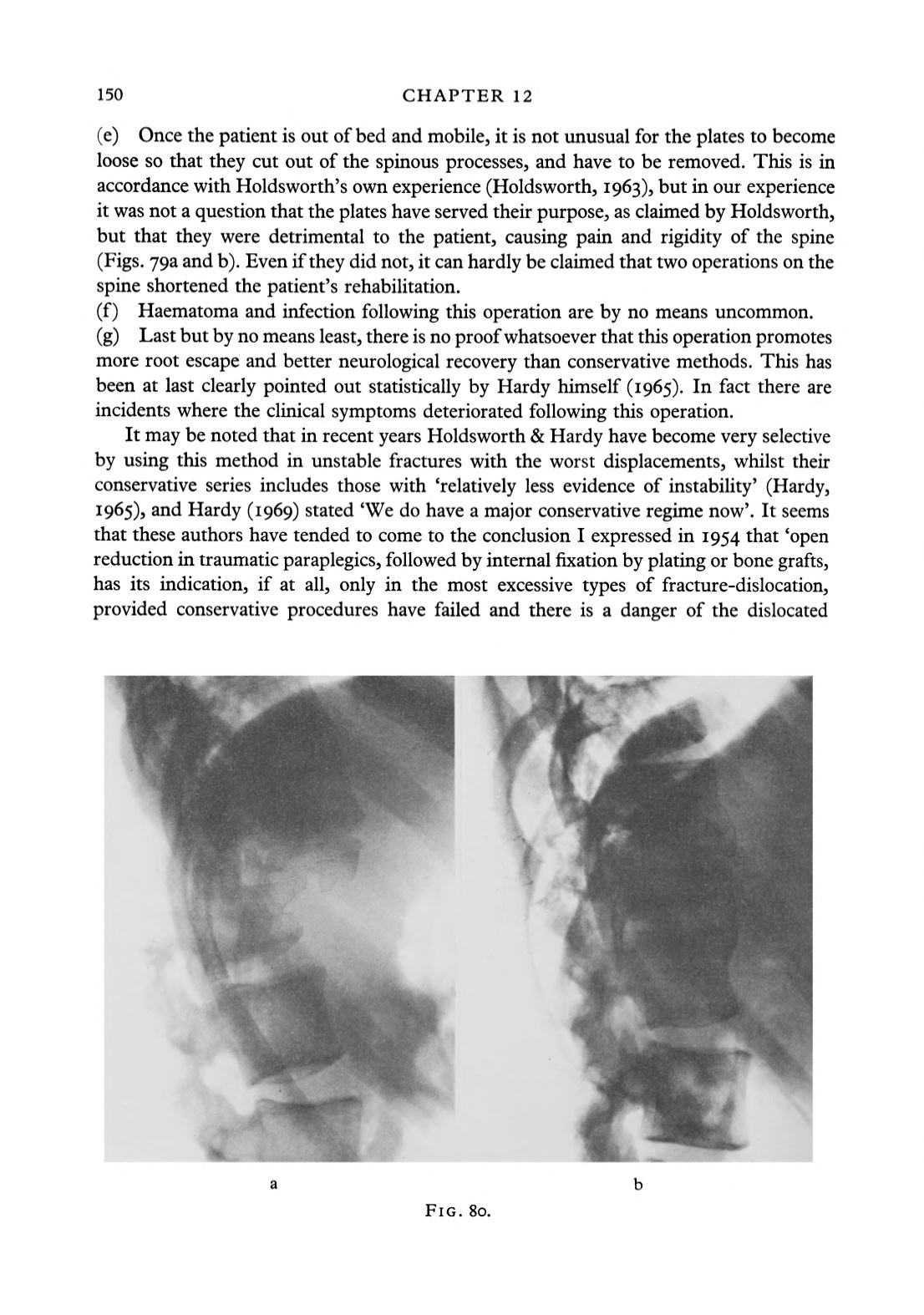
it was not a question that the plates have served their purpose, as claimed by Holdsworth,
but that they were detrimental to the patient, causing pain and rigidity of the spine
(Figs. 793 and b). Even if they did not, it can hardly be claimed that two operations on the
spine shortened the patient's rehabilitation.
(f) Haematoma and infection following this operation are by no means uncommon.
(g) Last but by no means least, there is no proofwhatsoever that this operation promotes
more root escape and better neurological recovery than conservative methods. This has
been at last clearly pointed out statistically by Hardy himself (1965). In fact there are
incidents where the clinical symptoms deteriorated following this operation.
It may be noted that in recent years Holdsworth & Hardy have become very selective
by using this method in unstable fractures with the worst displacements, whilst their
conservative series includes those with 'relatively less evidence of instability' (Hardy,
1 965)3 and Hardy (1969) stated 'We do have a major conservative regime now'. It seems
that these authors have tended to come to the conclusion I expressed in 1954 that 'open
reduction in traumatic paraplegics, followed by internal fixation by plating or bone grafts,
has its indication, if at all, only in the most excessive types of fracture-dislocation,
provided conservative procedures have failed and there is a danger of the dislocated
FIG. 80.


