F- CLINICAL ASPECTS OF SPINAL CORD INJURIES
347
agreed that in the management of spinal cord injuries intermittent catheterization
drainage is the worst form of treatment which can be used'.
I have always considered intermittent catheterization in the acute stages of paraplegia
and tetraplegia as a major medical and not a nursing procedure. It should, therefore, be
carried out exclusively both in men and women by a medical officer familiar with the
non-touch technique and not left to the nursing staff, let alone to orderlies or 'tech
nicians'. Over the years, this concept has been consistently adhered to, and intermittent
catherization has continued to be the method of choice in the management of the paralysed
bladder during the caute stages of paraplegia and tetraplegia. It has been found, that by
using this regime the paralysed bladder can be kept sterile in the great majority of
patients not only for many weeks but indeed often throughout the whole period that
catheterization has been needed. I am, of course, aware that other workers in this field,
even some in spinal units, would argue that they have not sufficient staff or time to carry
out intermittent catheterization and revert to the immediate method of urethral drainage
by an indwelling catheter. However, I cannot accept such arguments as valid in this field
of medicine since they are not acceptable in any other field by our profession. It must be
stressed that the time taken in carrying out the technique of intermittent catheterization
with all its meticulous care, is well spent in preventing the disastrous complications
associated with ascending infection of the urinary tract resulting in chronic invalidism
and early death of these unfortunate people. This is particularly vital in those patients
who, in addition to the spinal injury, have associated injuries to the chest and other parts
of the body, where the organism has to deal with all the potential complications of these
injuries and, no doubt, it can do so more readily, if it is not interfered with by an additional
infection of the urinary tract.
Immediate indwelling catheterization may be indicated for the determination of
osmolal output in acute renal failure following acute traumatic paraplegia. This is now
very rare.
Technique and procedure
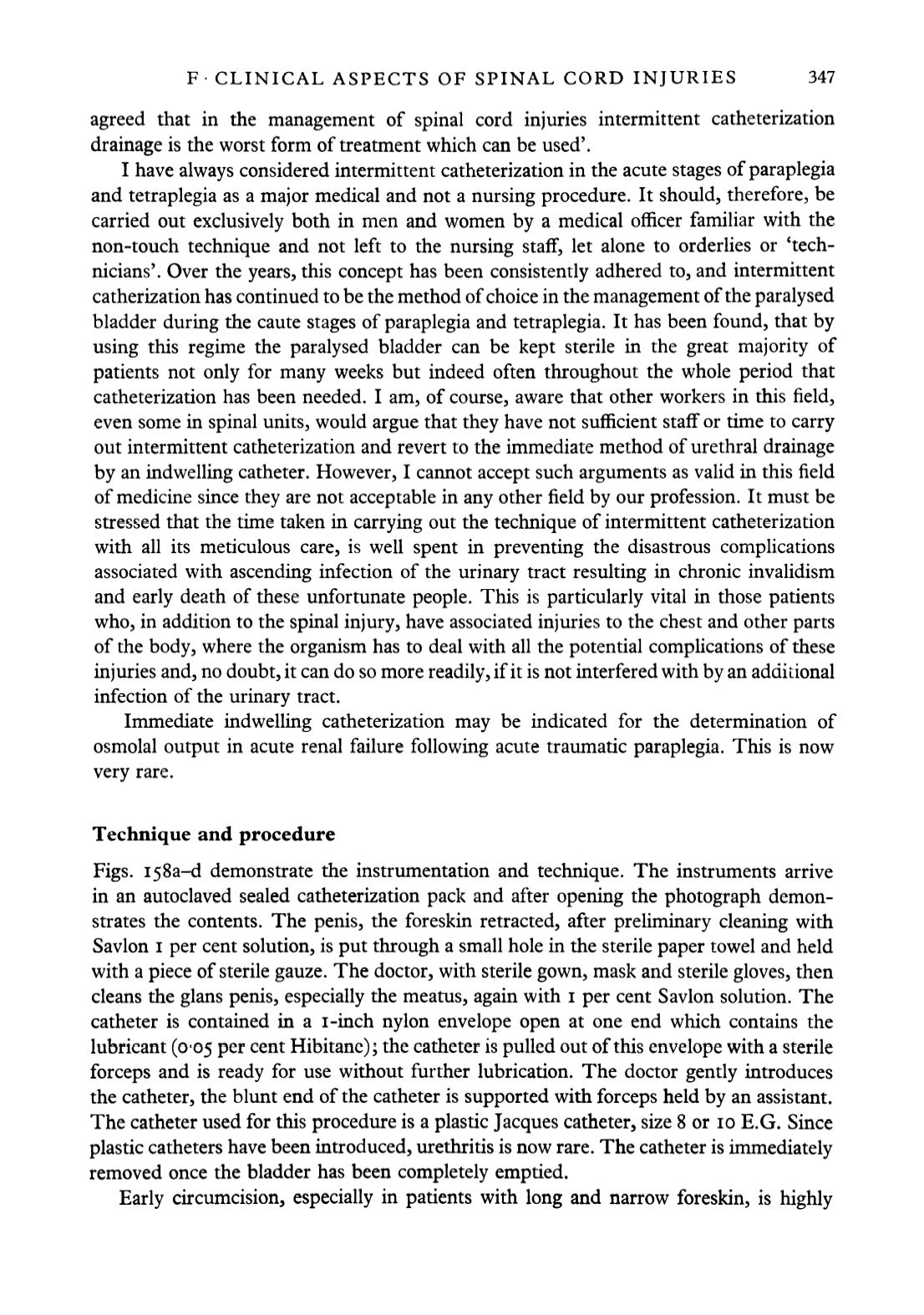
Figs. ifSa-d demonstrate the instrumentation and technique. The instruments arrive
in an autoclaved sealed catheterization pack and after opening the photograph demon
strates the contents. The penis, the foreskin retracted, after preliminary cleaning with
Savlon i per cent solution, is put through a small hole in the sterile paper towel and held
with a piece of sterile gauze. The doctor, with sterile gown, mask and sterile gloves, then
cleans the glans penis, especially the meatus, again with i per cent Savlon solution. The
catheter is contained in a i-inch nylon envelope open at one end which contains the
lubricant (0-05 per cent Hibitane); the catheter is pulled out of this envelope with a sterile
forceps and is ready for use without further lubrication. The doctor gently introduces
the catheter, the blunt end of the catheter is supported with forceps held by an assistant.
The catheter used for this procedure is a plastic Jacques catheter, size 8 or 10 E.G. Since
plastic catheters have been introduced, urethritis is now rare. The catheter is immediately
removed once the bladder has been completely emptied.
Early circumcision, especially in patients with long and narrow foreskin, is highly


