CLINICAL ASPECTS OF SPINAL CORD INJURIES
T4 lesion, cooling
____T4 lesion, heating
287
.27 C.
18-20'C
37.o
35
33h
_ 31
u
^29;
.
E27r
<u
I
I-
25
23
21 r-
•0--0--0---
°
- o--- -o-- - -o Rectum
-"Forehead
>-vx' ^-t- Side
^~
~&\o-
Chest above
lesion
•-Chest below
lesion
/
\-v
N A\
19
\
^' ^ ^
Finger
\ Toe
27 C
35-37°C
1
2
Tune (hr)
3
0
FIG. 1246.
1
2
Time (hr)
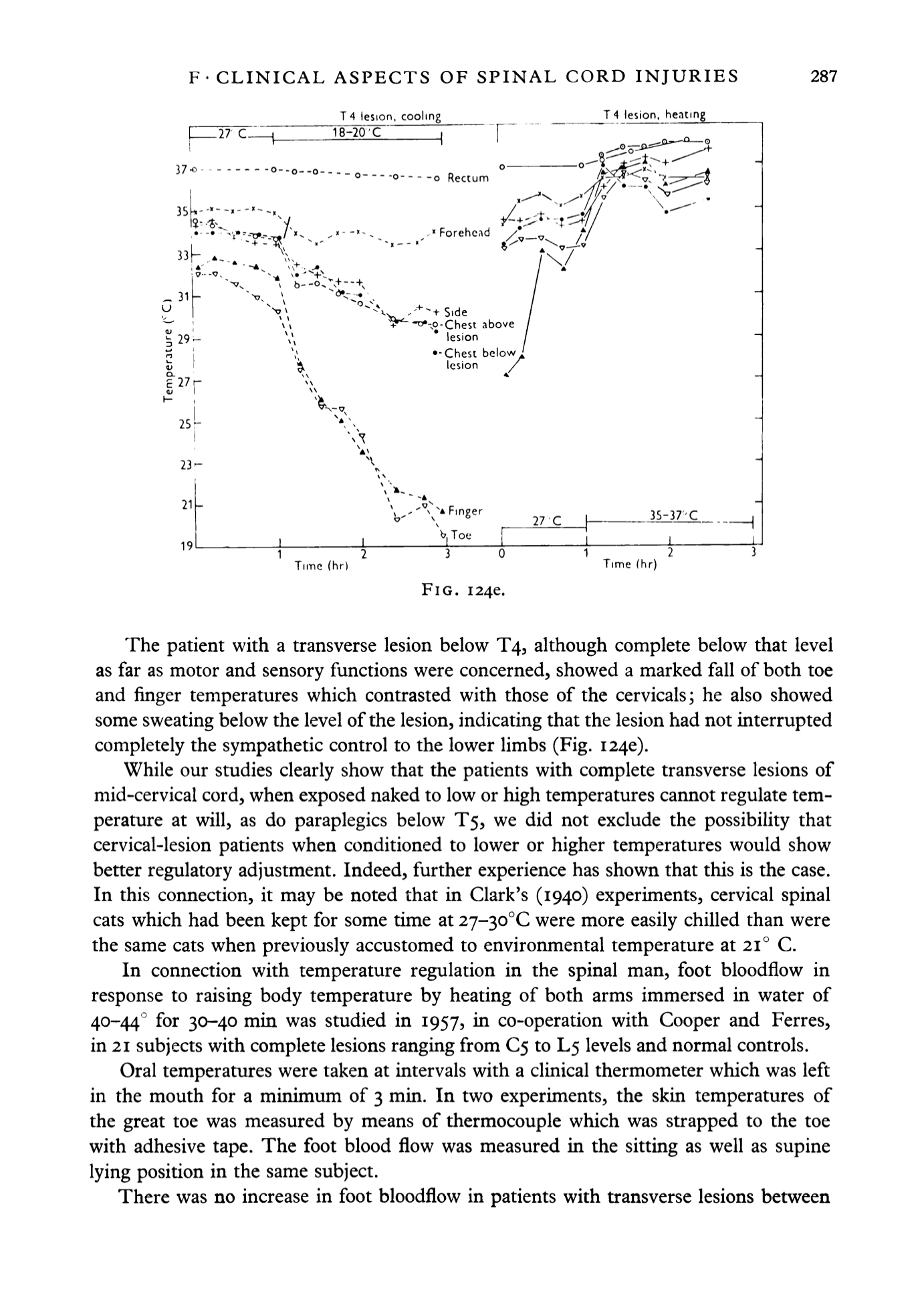
The patient with a transverse lesion below T4, although complete below that level
as far as motor and sensory functions were concerned, showed a marked fall of both toe
and finger temperatures which contrasted with those of the cervicals; he also showed
some sweating below the level of the lesion, indicating that the lesion had not interrupted
completely the sympathetic control to the lower limbs (Fig.
1240).
While our studies clearly show that the patients with complete transverse lesions of
mid-cervical cord, when exposed naked to low or high temperatures cannot regulate tem
perature at will, as do paraplegics below T5, we did not exclude the possibility that
cervical-lesion patients when conditioned to lower or higher temperatures would show
better regulatory adjustment. Indeed, further experience has shown that this is the case.
In this connection, it may be noted that in Clark's (1940) experiments, cervical spinal
cats which had been kept for some time at
2j-^o°C
were more easily chilled than were
the same cats when previously accustomed to environmental temperature at 21° C.
In connection with temperature regulation in the spinal man, foot bloodflow in
response to raising body temperature by heating of both arms immersed in water of
40-44° for 30-40 min was studied in 1957, m co-operation with Cooper and Ferres,
in
21
subjects with complete lesions ranging from
€5
to L5 levels and normal controls.
Oral temperatures were taken at intervals with a clinical thermometer which was left
in the mouth for a minimum of 3 min. In two experiments, the skin temperatures of
the great toe was measured by means of thermocouple which was strapped to the toe
with adhesive tape. The foot blood flow was measured in the sitting as well as supine
lying position in the same subject.
There was no increase in foot bloodflow in patients with transverse lesions between


