F- CLINICAL ASPECTS OF SPINAL CORD INJURIES
333
This was in contrast to only slight rise of venous pressure and insignificant changes in
blood pressure and pulse, in spite of vigorous detrusor contractions raising the bladder
pressure to over 60 cm H2O, in all lesions below T6, as in the low lesions the vascular
bed above the cord transection is large enough for compensatory distribution of blood
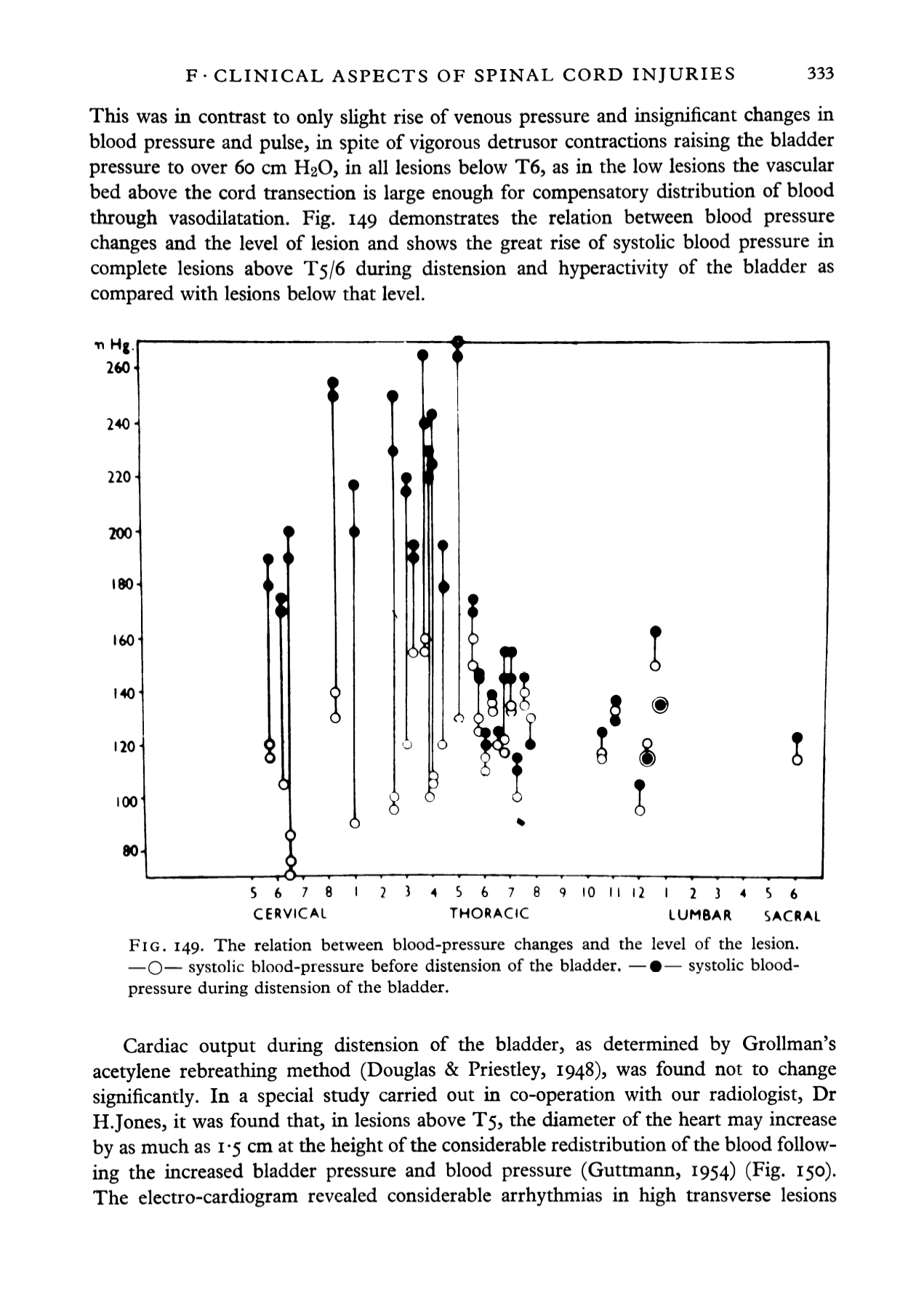
through vasodilatation. Fig. 149 demonstrates the relation between blood pressure
changes and the level of lesion and shows the great rise of systolic blood pressure in
complete lesions above T5/6 during distension and hyperactivity of the bladder as
compared with lesions below that level.
•n Hg
260'
240-
220-
200
180
160
140
120
100
80
i
I
8
)
O
i
S
6
7
8
I
2
CERVICAL
56 78 9
10
II 12
I
23
4
$6
THORACIC
LUMBAR
SACRAL
FIG. 149. The relation between blood-pressure changes and the level of the lesion.
—O— systolic blood-pressure before distension of the bladder. —•— systolic blood-
pressure during distension of the bladder.
Cardiac output during distension of the bladder, as determined by Grollman's
acetylene rebreathing method (Douglas & Priestley, 1948), was found not to change
significantly. In a special study carried out in co-operation with our radiologist, Dr
H.Jones, it was found that, in lesions above TS, the diameter of the heart may increase
by as much as 1-5 cm at the height of the considerable redistribution of the blood follow
ing the increased bladder pressure and blood pressure (Guttmann, 1954) (Fig. 150).
The electro-cardiogram revealed considerable arrhythmias in high transverse lesions


