B - ANATOMY, NEUROPATHOLOGY AND REGENERATION
77
pressure of 145 mm and complete block. He was put on respirator and head traction.
He died 3 days later from a total collapse of the right lung due to mucuous plugging.
The findings in this case are shown in Figs. 34a-f. The segments C6 and
Cj
show com–
plete disintegration of the normal architecture of the cord and disappearance of the
distinction between the grey and white substances. The whole shape of the segments is
distorted and the neural tissues are replaced by necrotic tissue intermingled with haemor–
rhages. There was a profound extension of the cord damage cephalad to C2 and caudal to
T5/6. Figs. 34a-f illustrate the effect of the concussion in caudal direction from C8 to T5
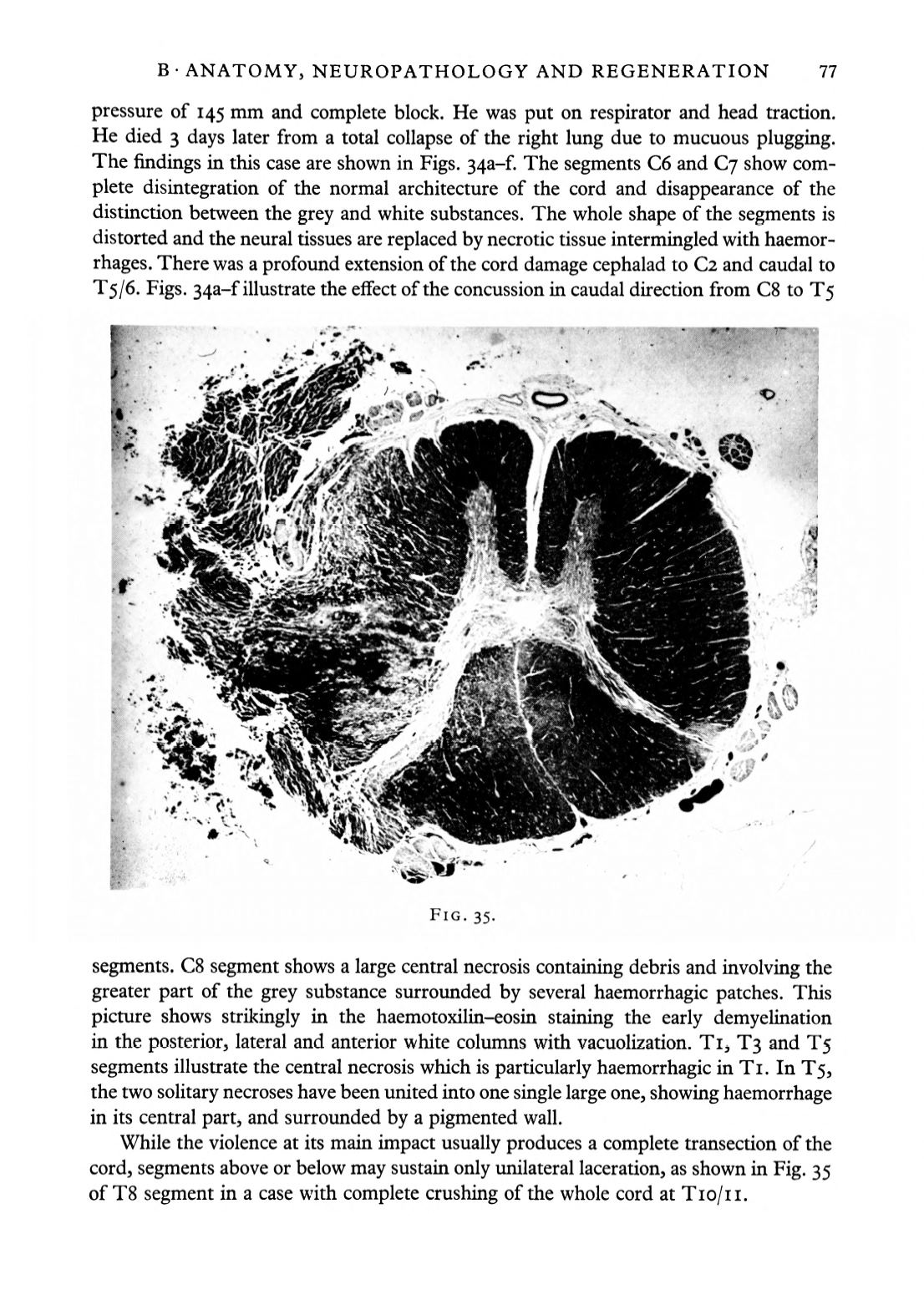
FIG. 35.
segments. C8 segment shows a large central necrosis containing debris and involving the
greater part of the grey substance surrounded by several haemorrhagic patches. This
picture shows strikingly in the haemotoxilin-eosin staining the early demyelination
in the posterior, lateral and anterior white columns with vacuolization. Ti, T3 and T5
segments illustrate the central necrosis which is particularly haemorrhagic in Ti. In T5,
the two solitary necroses have been united into one single large one, showing haemorrhage
in its central part, and surrounded by a pigmented wall.
While the violence at its main impact usually produces a complete transection of the
cord, segments above or below may sustain only unilateral laceration, as shown in Fig. 35
of T8 segment in a case with complete crushing of the whole cord at TIO/II.


